Source: www.ocregister.com/ocregister/ news/atoz/article_934357.php
The Morning Read: Bringing health home
Doctor takes a personal approach to patients, hauling his office to their living rooms.
This is not your typical doctor's office. The room is dim. The air reeks of stale cigarette smoke. When you sit on the sofa, a cloud of dust rises up. And the scale on the floor is 6 pounds off.
But today, for close to an hour, Bob Price's apartment in San Clemente is a doctor's office. Norm Vinn's office, to be precise.
You don't go to Vinn. Vinn comes to you. He is one of maybe a dozen physicians in Orange County whose business is making house calls.
While your family practitioner might squeeze in 20 to 30 patients a day, Vinn sees eight. While your family practitioner might see you for 15 to 30 minutes, Vinn listens for up to an hour.
"I don't want to get too weepy here," he says over a cup of steaming coffee at a booth at Denny's, his office this morning. But trading in his family practice for the slower-paced house-call track was a chance "to find some inner peace. And spiritual fulfillment."
He was sick of always being in "too much of a hurry to ask people about the book they're reading or their families," he says.
By 9 a.m. on most days, Vinn is finished surfing Lower Trestles and is driving to his first visit in his silver Lexus.
Today he stops on a street in San Clemente, fishes a stethoscope, doctor kit and miniature lab-test machine out of his trunk and walks up to the door of Apartment A with a knock and a holler. "Bob? It's Dr. Vinn!"
Inside, Bob Price is lying on his side in bed, his skinny legs barely covered by a loose blue hospital gown. There's no bottom sheet on the mattress. His feet are bare.
"No hair, no teeth, no aorta," is how Price sums up his condition. An aneurysm blew the aorta out and he's had prostate cancer for 11 years, not to mention "two bad hips and two bad legs," scoliosis, arthritis, a cold that won't quit, a rash, congestion and a creeping cataract.
But Price is an optimist. "Eighty-five and still alive!" he laughs.
Vinn "has been a godsend," Price says.
Price doesn't have a wife or children or a car, and even if he did own wheels he can barely hobble to the bathroom a few feet from his bed, let alone drive to a doctor.
He is the prototypical house-call patient. Medicare requires that it take "significant and taxing effort" for the patient to walk 100 feet before it will pay for a house call.
Vinn's patients include a young woman who was paralyzed in a freeway wreck and a man who can't get out of bed because he weighs more than 700 pounds. But most people he treats are in their 80s, trapped in their homes because their bodies are just calling it quits.
Just as often as Vinn discusses a patient's blood pressure, he finds himself discussing their mortality. Are they ready? How are they coping? "Candid, strange conversations," he says. If dementia is present, that conversation is often with the patient's spouse or children.
Because most of his patients are facing The End, the depression factor is one of the downsides of the house-call business. It brings to his mind the axiom: When you're a hammer, everything starts looking like a nail.
So when he starts feeling like everyone is dying, he takes off his red tie and white button-down shirt, puts on a wetsuit and heads to the ocean to put things back into perspective.
Vinn opened his practice in Long Beach in 1978 and enjoyed it until managed care came along in the '80s. The turnstile of patients, he said, became "very frustrating for patients and very frustrating for the doctors."
Vinn is an osteopathic physician, which means he treats the whole person. Besides diagnosing illnesses and treating symptoms, he counsels patients on nutrition and hygiene, addresses depression and loneliness, discusses financial hardships and even connects patients with social-service agencies.
In other words, he needs more than 20 minutes.
It got to a point where he was coming home at night to his wife and three daughters, "angry, irritable, frustrated, depressed. I wondered if I was a squirrel in a cage."
In 1998 Medicare began paying doctors more equitably to make house calls, Vinn says. The next year a colleague told Vinn about a doctor who had started a house-call business in San Diego. Vinn took a chance and joined the group. In 2002 he started his own business called Housecall Doctors Medical Group.
He brought in another doctor and three nurse practitioners and opened an office in Laguna Hills, but it's only used to store charts.
Not being chained to an office has its perks, but it also has a few hassles. Vinn puts 2,500 miles a month on his car driving to patients all over Orange County. He earns about 20 percent less than when he had an office practice. He meets medical officials in parking lots to sign death certificates and gets calls from patients at all hours.
The other night, a call came during dinner from a woman who got his number from a health-care agency. Vinn told her he was eating and would be there as soon as possible. By the time he showed up at her house, she said she was having her dinner and refused to let him in.
But most of the 350 patients in his practice are so appreciative, they practically gush.
Price says he is grateful that Vinn is simply around to talk to. And Price is quite a talker.
Now he is talking about how he never considered giving up smoking because he thinks it's therapeutic for people who experience depression. Vinn sticks a flu shot into Price's arm. Then he checks his prostate.
"Thank you, sir," Price says when it's done.
"Are you eating a lot? You look to me like your face is thinner," Vinn says.
"You think you can weigh me?" Price asks. "That's a good idea, doctor."
Price swings his legs around to sit on the bed. Then, leaning on his walker, he stands and steps precariously onto an old dusty scale that the doctor brought in from the kitchen. Letting go of his walker, Price balances for a few shaky seconds to put his full weight on the scale. It reads 127 pounds.
"I weighed 185!" Price says. "Well, stranger things have happened."
"Let's try it one more time," says the doctor.
The room is dim, maybe they read it wrong. "You want a flashlight?" Price asks.
Vinn says no but steps on the scale himself to check for accuracy. It's about 6 pounds light, he decides. When Price steps back on, it still registers 127. So he's probably 133 pounds, the doctor figures.
"Oh, man. If I had any sense, I'd be scared," Price says.
Six days later Price calls an ambulance to take him to a hospital in Long Beach. He can't manage his catheter anymore. Vinn gets wind of it, rings a San Clemente rest home and asks them to hold a bed for Price so he can bring him back to Orange County.
"That way Dr. Vinn can still look in on me," Price says. "Ya know. I think everything's gonna be fine."
Friday, January 06, 2006
Wednesday, January 04, 2006
Curing Shoulder Pain Using Osteopathic Manipulative Treatment(OMT) by DOs
Source: www.indiangyan.com/books/therapybooks/ Osteopathy/Curing_Shoulder_pain.shtml
'Doctor, I don't know what has happened to my shoulders. They ache a lot and the ache is gradually increasing. I cannot move them properly. It is becoming impossible for me to put on my clothes myself even combing has to be done by somebody else. The pain persists during the day, but at night it becomes worse. If somebody presses my shoulder joint, I get an excruciating pain. I have had all kinds of treatment but nothing seems to be helping me. Can you do something?'
The above symptoms seemed to point towards a frozen shoulder. This condition can be diagnosed easily. The shoulder joint is frozen and its mobility reduced. Before we go further let us examine what our shoulder joints are and what they do.
A shoulder joint is a ball and a socket joint. The head of the upper arm bone (humerus) and a shallow cup-like structure of the shoulder blade (scapula) make up this joint. The head is much bigger than the socket and only a part of the head can fit into the socket called the glenoid cavity. The socket is deepened by a fibrocartilagenous rim. Due to this arrangement, the shoulder has a better range of movement than any other joint in the body. But it is a weak joint and depends on the surrounding muscles for its strength.
The joint is covered by a sac-like structure, a fibrous capsule. This capsule is lax and the bones can be separated from each other for a distance upto half an inch. This can provide a further range of movement. The inferior part of the capsule is the weakest part. The movement at the shoulder joint is further increased by the movement of the shoulder blade itself When the arm is raised upto 1200, movement takes place at the shoulder joint and a further 600 is obtained by rotation of the shoulder blade. The acromio-clavicular joint at the lateral end of the collarbone (clavicle) and sterno-clavicular joint at the medial end of the collarbone also participate in shoulder movements.
In the case of a frozen shoulder, the capsule is thickened and retracted. This can be clearly demonstrated by orthography (taking an X-ray after injecting a radio-opaque dye inside the joint).
Why a frozen shoulder occurs is not known. There is a limitation of movement in all directions. It generally occurs between the ages of forty-to-sixty. After sixty, it is rare. The usual course of the disease is as follows:
It starts with an ache in the shoulder when the arm is moved. There is pain when the arm is kept still. After one month the pain is more severe and spreads down to the elbow. It is worse at night and increases further if the patient lies on the same side. Restriction of movement starts becoming obvious. After 2-3 months severe pain occurs at the slightest movement. The patient cannot raise his hand more than thirty to forty degrees. The rotative movement of the arm is also limited. After 4 months no further diminution takes place in the movement. The pain is at its worst at the end of 4 months. After 5 months it begins to reduce gradually. After 6 months there is no constant pain. Pain is felt only when the arm is moved. The patient is now able to lie on the painful side. After 7 months there is pain only in the upper part of the shoulder. After 8 months the range of movement begins to become wider. After one year the patient is almost well.
It has been noted that the pain and restriction of movement decrease during the first four months. During the next four months the pain decreases but the limitation of movement persists. In the last 4 months the range of movement returns. If exercises are done, the full range of movement is sure to return, and if no exercises are done, some amount of permanent limitation will persist at the shoulder joint.
In the severe variety, pain may go on increasing upto nine months. Wasting and thinning of muscles also start and complete recovery may take upto two years.
Treatment
Some doctors advise forced mobilization under general anesthesia. Though some very good results have been achieved by this process, some grave setbacks also occur. This treatment is therefore not advisable because during this act a tear in the lower part of the capsule can occur. This has been seen by orthography taken before and after the treatment. We believe that skill and experience play a dominant role in achieving good results. It is very important to know when to stop and how to grade these maneuvers. This is practically impossible when the manipulation is done under anesthesia, because the results are only known the next day or when the patient wakes up. For such cases we recommend a gradual stretching of the shoulder without anesthesia. However this is not as simple as it sounds. If there is too much stretching, it provokes pain and if there is too little, it does not produce any results. Stretching has to be done with great care. The patient feels great discomfort when the arm reaches the restricted range; it should then be coaxed a little further without increasing the pain or producing a muscle spasm. The shoulder should be moved in this final increased range for five to seven minutes twice a week. The patient should also be taught certain exercises which should be done twice a day at home. This treatment, in my experience, reduces the recovery period to two to three months. Sometimes cervical and upper dorsal manipulation along with mobilization is helpful.
This treatment can also be given in the case of a frozen shoulder after an accident.
There are other cases where the patient feels pain in the shoulder joint, but it is radiated from the neck. In these cases, 'the shoulder is nothing, the neck is everything!' Here manipulation of the lower cervical spine brings about a spectacular recovery, and when this is so, the above diagnosis is confirmed. In these cases movement at the shoulder joint is quite free. Pain may radiate in the whole arm from the base to the neck, accompanied by numbness, a tingling sensation and a feeling of pins and needles in the hands.
The pain in the shoulder may also be caused by diseases of the thorax and abdomen.
Exercises
Keeping the joint mobile is very important. This can be done at home in the following way:
1. Stand up, bend forward, leave your arm hanging loose, take it to the right as far as you can, then to the left. Then take it forward and backward. Rotate the arm clockwise and anti-clockwise. Repeat this twenty times. (Fig. 40, A & B).
2. Stand by the side of the wall, with your affected shoulder on the wall side. Now bend your arm at the elbow. Rest the forearm on a platform by the wall as high as possible. Bend your knees and slowly come down. As you come down you will stretch your shoulder up. Go down as far as you can and then come up. Repeat this twenty times (Fig. 40, C).
Case Histories
@ A fifty-five-year old man had pain in his right shoulder and his movement was restricted for five months. He had no history of injury. The pain in the right shoulder went on increasing. Along with doing exercises, he took diathermy and intra-articular hydro-cortisone injections, but nothing helped.
He came to me with this complaint. The X-ray of his shoulder joint was clear: the cervical spine showed spondylosis. The blood sugar was high. He could not raise his arm more than forty-five degrees.
Manipulative treatment was started and he was called twice a week. He was taught a few exercises to be done at home. By the end of three weeks, he could raise his arm to about 1200. Treatment continued for two months and he was ninety per cent better. He was advised to continue exercises and come fortnightly for treatment. Two months later he was completely free of pain.
@ A thirty-eight-year old man, thinly built, had a severe pain in the left shoulder radiating to the arm, with a tingling sensation in the left hand. He had had a similar attack a year before which had cleared in two months. He took anti-inflammatory drugs which gave him little relief He consulted orthopaedic surgeons and an X-ray was taken, confirming that he had spondylosis of the cervical spine.
Manipulative treatment was started. Following the treatment he had no pain for four days. He was cured after the third round of manipulative treatment.
'Doctor, I don't know what has happened to my shoulders. They ache a lot and the ache is gradually increasing. I cannot move them properly. It is becoming impossible for me to put on my clothes myself even combing has to be done by somebody else. The pain persists during the day, but at night it becomes worse. If somebody presses my shoulder joint, I get an excruciating pain. I have had all kinds of treatment but nothing seems to be helping me. Can you do something?'
The above symptoms seemed to point towards a frozen shoulder. This condition can be diagnosed easily. The shoulder joint is frozen and its mobility reduced. Before we go further let us examine what our shoulder joints are and what they do.
A shoulder joint is a ball and a socket joint. The head of the upper arm bone (humerus) and a shallow cup-like structure of the shoulder blade (scapula) make up this joint. The head is much bigger than the socket and only a part of the head can fit into the socket called the glenoid cavity. The socket is deepened by a fibrocartilagenous rim. Due to this arrangement, the shoulder has a better range of movement than any other joint in the body. But it is a weak joint and depends on the surrounding muscles for its strength.
The joint is covered by a sac-like structure, a fibrous capsule. This capsule is lax and the bones can be separated from each other for a distance upto half an inch. This can provide a further range of movement. The inferior part of the capsule is the weakest part. The movement at the shoulder joint is further increased by the movement of the shoulder blade itself When the arm is raised upto 1200, movement takes place at the shoulder joint and a further 600 is obtained by rotation of the shoulder blade. The acromio-clavicular joint at the lateral end of the collarbone (clavicle) and sterno-clavicular joint at the medial end of the collarbone also participate in shoulder movements.
In the case of a frozen shoulder, the capsule is thickened and retracted. This can be clearly demonstrated by orthography (taking an X-ray after injecting a radio-opaque dye inside the joint).
Why a frozen shoulder occurs is not known. There is a limitation of movement in all directions. It generally occurs between the ages of forty-to-sixty. After sixty, it is rare. The usual course of the disease is as follows:
It starts with an ache in the shoulder when the arm is moved. There is pain when the arm is kept still. After one month the pain is more severe and spreads down to the elbow. It is worse at night and increases further if the patient lies on the same side. Restriction of movement starts becoming obvious. After 2-3 months severe pain occurs at the slightest movement. The patient cannot raise his hand more than thirty to forty degrees. The rotative movement of the arm is also limited. After 4 months no further diminution takes place in the movement. The pain is at its worst at the end of 4 months. After 5 months it begins to reduce gradually. After 6 months there is no constant pain. Pain is felt only when the arm is moved. The patient is now able to lie on the painful side. After 7 months there is pain only in the upper part of the shoulder. After 8 months the range of movement begins to become wider. After one year the patient is almost well.
It has been noted that the pain and restriction of movement decrease during the first four months. During the next four months the pain decreases but the limitation of movement persists. In the last 4 months the range of movement returns. If exercises are done, the full range of movement is sure to return, and if no exercises are done, some amount of permanent limitation will persist at the shoulder joint.
In the severe variety, pain may go on increasing upto nine months. Wasting and thinning of muscles also start and complete recovery may take upto two years.
Treatment
Some doctors advise forced mobilization under general anesthesia. Though some very good results have been achieved by this process, some grave setbacks also occur. This treatment is therefore not advisable because during this act a tear in the lower part of the capsule can occur. This has been seen by orthography taken before and after the treatment. We believe that skill and experience play a dominant role in achieving good results. It is very important to know when to stop and how to grade these maneuvers. This is practically impossible when the manipulation is done under anesthesia, because the results are only known the next day or when the patient wakes up. For such cases we recommend a gradual stretching of the shoulder without anesthesia. However this is not as simple as it sounds. If there is too much stretching, it provokes pain and if there is too little, it does not produce any results. Stretching has to be done with great care. The patient feels great discomfort when the arm reaches the restricted range; it should then be coaxed a little further without increasing the pain or producing a muscle spasm. The shoulder should be moved in this final increased range for five to seven minutes twice a week. The patient should also be taught certain exercises which should be done twice a day at home. This treatment, in my experience, reduces the recovery period to two to three months. Sometimes cervical and upper dorsal manipulation along with mobilization is helpful.
This treatment can also be given in the case of a frozen shoulder after an accident.
There are other cases where the patient feels pain in the shoulder joint, but it is radiated from the neck. In these cases, 'the shoulder is nothing, the neck is everything!' Here manipulation of the lower cervical spine brings about a spectacular recovery, and when this is so, the above diagnosis is confirmed. In these cases movement at the shoulder joint is quite free. Pain may radiate in the whole arm from the base to the neck, accompanied by numbness, a tingling sensation and a feeling of pins and needles in the hands.
The pain in the shoulder may also be caused by diseases of the thorax and abdomen.
Exercises
Keeping the joint mobile is very important. This can be done at home in the following way:
1. Stand up, bend forward, leave your arm hanging loose, take it to the right as far as you can, then to the left. Then take it forward and backward. Rotate the arm clockwise and anti-clockwise. Repeat this twenty times. (Fig. 40, A & B).
2. Stand by the side of the wall, with your affected shoulder on the wall side. Now bend your arm at the elbow. Rest the forearm on a platform by the wall as high as possible. Bend your knees and slowly come down. As you come down you will stretch your shoulder up. Go down as far as you can and then come up. Repeat this twenty times (Fig. 40, C).
Case Histories
@ A fifty-five-year old man had pain in his right shoulder and his movement was restricted for five months. He had no history of injury. The pain in the right shoulder went on increasing. Along with doing exercises, he took diathermy and intra-articular hydro-cortisone injections, but nothing helped.
He came to me with this complaint. The X-ray of his shoulder joint was clear: the cervical spine showed spondylosis. The blood sugar was high. He could not raise his arm more than forty-five degrees.
Manipulative treatment was started and he was called twice a week. He was taught a few exercises to be done at home. By the end of three weeks, he could raise his arm to about 1200. Treatment continued for two months and he was ninety per cent better. He was advised to continue exercises and come fortnightly for treatment. Two months later he was completely free of pain.
@ A thirty-eight-year old man, thinly built, had a severe pain in the left shoulder radiating to the arm, with a tingling sensation in the left hand. He had had a similar attack a year before which had cleared in two months. He took anti-inflammatory drugs which gave him little relief He consulted orthopaedic surgeons and an X-ray was taken, confirming that he had spondylosis of the cervical spine.
Manipulative treatment was started. Following the treatment he had no pain for four days. He was cured after the third round of manipulative treatment.
Sunday, January 01, 2006
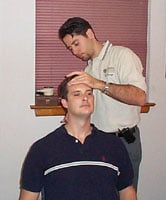
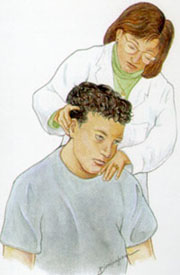
Cervical Mobilization in Post Traumatic Headache/Cervicalgia
Source: www.birf.info/home/library/ alt-med/altmedlib_cervmob.html
By Sherman Gorbis, DO, FAAO
All osteopathic physicians, in their first two years of osteopathic medical college training, are taught Osteopathic Palpatory Diagnosis and Osteopathic Manipulative Treatment (OMT). OMT is one type of manual medicine. OMT is defined as “The therapeutic application of manually guided forces by an osteopathic physician to improve physiologic function and/or support homeostasis that have been altered by somatic dysfunction” (1). Somatic dysfunction is defined as “Impaired or altered function of related components of the somatic (body framework) system: skeletal, arthrodial, and myofascial structures, and related vascular, lymphatic, and neural elements.” Somatic dysfunction is treated using OMT (1).
The diagnostic triad for diagnosing somatic dysfunction is ART:
Asymmetry-determined visually and by palpation
Restriction of motion-determined by palpation
Tissue texture abnormality-determined by palpation
Traumatic cervicalgia (neck pain) can occur as a result of a motor vehicle accident (commonly during/after a whiplash injury where the head and neck are thrown forward/backward), sports related injury, or a fall (such as from a ladder, horse, etc).
It would be very common and not un-expected for the patient who has experienced trauma to have Post Traumatic Headache/Cervicalgia (neck pain) with accompanying somatic dysfunction in her/his cervical spine (bones that make up the neck). The cervical spine is divided into two regions based on their motion characteristics:
Atypical cervical vertebrae. This includes C0-C2 (the upper surface of C2). C0 is the occipital bone, which is located in the lower back area of the skull. The occiput articulates (joined together to allow motion between them) with the first cervical vertebra, C1. C1 articulates with the second cervical vertebra, C2. Several muscles that have attachments in the cervical spine, or below, also attach to the occiput. When these muscles become hypertonic (a sustained contraction but not a spasm (as with a ‘charley horse'), headache can occur. If restriction of motion is present between vertebrae, due to a disruption in the motion of the facets (small joints between the vertebrae which have pain generators) neck pain and headache can occur.
The headache may also result from irritation of the right and/or left greater occipital nerve. This travels through the articulation between the occiput and the first cervical vertebra. It then travels up behind the ear and forward along the temple.
Typical cervical vertebrae.
This includes C2-T1 (the lower surface of C2-the upper surface of T1). As above, both muscle hypertonicity and motion restriction can lead to headache and neck pain
Once a physician evaluates the patient who has been involved in trauma and he/she has determined that no contraindications (special conditions that render the use of the procedure inadvisable, usually due to risk) exist for manual medicine, the manual medicine provider then has several options.
Various types of OMT include:
Soft tissue. This refers is directed toward tissues other than bone or joints (1).
Muscle energy. The patient voluntarily moves the body as specifically directed by the operator; this is from a precisely controlled position against a defined resistance by the operator (1). Muscle energy is, for the most part, directed at loosening tight muscles using isometric (the muscle does not shorten during the contraction) contractions of the affected muscles. It is also directed at providing proper motion of the facet joints between the vertebrae. Facet joints are located both on the inferior and superior surfaces of vertebrae to allow one vertebra to move freely in relation to the vertebra below. Muscle energy techniques can treat facets that are either dysfunctionally ‘opened' or ‘closed'.
Direct Action Thrust (Mobilization with Impulse). Uses a high-velocity/low-amplitude activation, or thrust, to move a joint that is experiencing somatic dysfunction to help restore appropriate physiologic motion (1). This can be, sometimes, accompanied by an audible ‘click' or ‘pop'. However, the goal of treatment is the restoration of motion, not the presence of the sound.
Myofascial Release. This approach engages continual palpatory (the provider's hands in contact with the patient) feedback to achieve release of myofascial (muscles and their soft tissue/fascial coverings) tissues. This can be employed when tissue hypertonicity is present without severe motion restriction.
Other types of OMT include functional indirect and cranio-sacral.
Many insurance companies cover OMT and many osteopathic physicians who include OMT in their practices accept these plans. It is always helpful for the patient to inquire with his/her insurance company, as well as the provider, regarding coverage.
Resources
Ward RC, exec. ed. Foundations for Osteopathic Medicine 2 nd ed. Philadelphia : Lippincott Williams & Wilkins, 2003.American Academy of Osteopathy (AAO) This group's mission is to teach, advocate, advance, explore, and research the science and art of osteopathic medicine, emphasizing osteopathic principles, philosophy, palpatory diagnosis and OMT in total health care. Most, if not all, members use OMT in some degree in their practices. Phone (317) 879-1881 Fax (317) 879-0563 www.academyofosteopathy.orgAmerican Osteopathic Association (AOA) Patients can inquire about educational materials regarding OMT. www.aoa-net.org
Sherman Gorbis, DO, FAAO is a graduate of the Kansas City (MO) College of Osteopathic Medicine . He interned at Riverside Osteopathic Hospital ( Trenton , MI ). He earned his certification in Osteopathic Manipulative Medicine (OMM) in 1991 and his Fellowship in the American Academy of Osteopathy (FAAO) in 1995. He is presently an Associate Professor in the Department of OMM at Michigan State University College of Osteopathic Medicine ( East Lansing , MI ).
By Sherman Gorbis, DO, FAAO
All osteopathic physicians, in their first two years of osteopathic medical college training, are taught Osteopathic Palpatory Diagnosis and Osteopathic Manipulative Treatment (OMT). OMT is one type of manual medicine. OMT is defined as “The therapeutic application of manually guided forces by an osteopathic physician to improve physiologic function and/or support homeostasis that have been altered by somatic dysfunction” (1). Somatic dysfunction is defined as “Impaired or altered function of related components of the somatic (body framework) system: skeletal, arthrodial, and myofascial structures, and related vascular, lymphatic, and neural elements.” Somatic dysfunction is treated using OMT (1).
The diagnostic triad for diagnosing somatic dysfunction is ART:
Asymmetry-determined visually and by palpation
Restriction of motion-determined by palpation
Tissue texture abnormality-determined by palpation
Traumatic cervicalgia (neck pain) can occur as a result of a motor vehicle accident (commonly during/after a whiplash injury where the head and neck are thrown forward/backward), sports related injury, or a fall (such as from a ladder, horse, etc).
It would be very common and not un-expected for the patient who has experienced trauma to have Post Traumatic Headache/Cervicalgia (neck pain) with accompanying somatic dysfunction in her/his cervical spine (bones that make up the neck). The cervical spine is divided into two regions based on their motion characteristics:
Atypical cervical vertebrae. This includes C0-C2 (the upper surface of C2). C0 is the occipital bone, which is located in the lower back area of the skull. The occiput articulates (joined together to allow motion between them) with the first cervical vertebra, C1. C1 articulates with the second cervical vertebra, C2. Several muscles that have attachments in the cervical spine, or below, also attach to the occiput. When these muscles become hypertonic (a sustained contraction but not a spasm (as with a ‘charley horse'), headache can occur. If restriction of motion is present between vertebrae, due to a disruption in the motion of the facets (small joints between the vertebrae which have pain generators) neck pain and headache can occur.
The headache may also result from irritation of the right and/or left greater occipital nerve. This travels through the articulation between the occiput and the first cervical vertebra. It then travels up behind the ear and forward along the temple.
Typical cervical vertebrae.
This includes C2-T1 (the lower surface of C2-the upper surface of T1). As above, both muscle hypertonicity and motion restriction can lead to headache and neck pain
Once a physician evaluates the patient who has been involved in trauma and he/she has determined that no contraindications (special conditions that render the use of the procedure inadvisable, usually due to risk) exist for manual medicine, the manual medicine provider then has several options.
Various types of OMT include:
Soft tissue. This refers is directed toward tissues other than bone or joints (1).
Muscle energy. The patient voluntarily moves the body as specifically directed by the operator; this is from a precisely controlled position against a defined resistance by the operator (1). Muscle energy is, for the most part, directed at loosening tight muscles using isometric (the muscle does not shorten during the contraction) contractions of the affected muscles. It is also directed at providing proper motion of the facet joints between the vertebrae. Facet joints are located both on the inferior and superior surfaces of vertebrae to allow one vertebra to move freely in relation to the vertebra below. Muscle energy techniques can treat facets that are either dysfunctionally ‘opened' or ‘closed'.
Direct Action Thrust (Mobilization with Impulse). Uses a high-velocity/low-amplitude activation, or thrust, to move a joint that is experiencing somatic dysfunction to help restore appropriate physiologic motion (1). This can be, sometimes, accompanied by an audible ‘click' or ‘pop'. However, the goal of treatment is the restoration of motion, not the presence of the sound.
Myofascial Release. This approach engages continual palpatory (the provider's hands in contact with the patient) feedback to achieve release of myofascial (muscles and their soft tissue/fascial coverings) tissues. This can be employed when tissue hypertonicity is present without severe motion restriction.
Other types of OMT include functional indirect and cranio-sacral.
Many insurance companies cover OMT and many osteopathic physicians who include OMT in their practices accept these plans. It is always helpful for the patient to inquire with his/her insurance company, as well as the provider, regarding coverage.
Resources
Ward RC, exec. ed. Foundations for Osteopathic Medicine 2 nd ed. Philadelphia : Lippincott Williams & Wilkins, 2003.American Academy of Osteopathy (AAO) This group's mission is to teach, advocate, advance, explore, and research the science and art of osteopathic medicine, emphasizing osteopathic principles, philosophy, palpatory diagnosis and OMT in total health care. Most, if not all, members use OMT in some degree in their practices. Phone (317) 879-1881 Fax (317) 879-0563 www.academyofosteopathy.orgAmerican Osteopathic Association (AOA) Patients can inquire about educational materials regarding OMT. www.aoa-net.org
Sherman Gorbis, DO, FAAO is a graduate of the Kansas City (MO) College of Osteopathic Medicine . He interned at Riverside Osteopathic Hospital ( Trenton , MI ). He earned his certification in Osteopathic Manipulative Medicine (OMM) in 1991 and his Fellowship in the American Academy of Osteopathy (FAAO) in 1995. He is presently an Associate Professor in the Department of OMM at Michigan State University College of Osteopathic Medicine ( East Lansing , MI ).
Treating a Whiplash with Osteopathic Manipulative Treatment(OMT)
Source: orthoinfo.aaos.org/fact/ thr_report.cfm?Thread_ID=232&topcategory=Neck
Imagine yourself driving when a car behind you rear-ends your vehicle. The impact pushes your car forward. It takes about 100 milliseconds for your body to catch up to the forward movement. Your shoulders travel forward until they are under your head, and your neck extends forward as your head tilts slightly down toward your steering wheel. You step on the brakes, bringing the car to an abrupt halt. The sudden stop throws your head and neck backward, and they bounce against the headrest. In a matter of seconds, you've experienced the classic mechanism of injury for whiplash.
About 20 percent of people involved in rear-end collisions later experience symptoms that center in the neck region. Although most of these people recover quickly, a small number develop chronic conditions that result in severe pain and sometimes disability.
Signs and symptoms
People who experience whiplash may develop one or more of the following symptoms, usually within the first two days after the accident:
Neck pain and stiffness
Headaches
Pain in the shoulder or between the shoulder blades
Low back pain
Pain or numbness in the arm and/or hand
Dizziness
Ringing in the ears or blurred vision
Difficulty concentrating or remembering
Irritability, sleep disturbances, fatigue
Diagnosis and Treatment
How whiplash injuries occur is clearly understood, but the extent and type of injuries varies greatly. The diagnosis of whiplash is often one of exclusion. Most injuries are to soft tissues such as the disks, muscles and ligaments, and cannot be seen on standard X-rays. Your doctor may need to request specialized tests, such as computed tomography scans or magnetic resonance imaging (MRI).
In the past, whiplash injuries were often treated with immobilization in a cervical collar. However, the current trend is to encourage early movement, rather than immobilization. The soft collar may be used for a short term and on an intermittent basis.
Ice may be applied for the first 24 hours, followed by gentle active movement. Your doctor may provide you with a series of exercises that you can do at home. An early return to work is encouraged, even if your doctor must prescribe some temporary modifications in your work situation. No single treatment has been scientifically proven as effective, but pain relieving medications, exercises, physical therapy, traction, massage, heat, ice, injections and ultrasound have all been beneficial for some patients.
As soon as possible, you should begin aerobic activities, such as walking. Your doctor may prescribe some isometric exercises as your condition improves. Symptoms resolve within several months for about 75 percent of people who have whiplash. Chronic conditions should be investigated further and might require surgery.
Where OMT comes in handy.....
OMTs can be applied to a variety of health problems, both musculoskeletal and non-musculoskeletal. According to the US Department of Health and Human Services, OMTs are most effective for back and neck pain. In fact, if you have back pain, you may be able to reduce the amount of pain medication you are taking if you receive OMT as part of your therapy. One study showed that patients with pancreatitis were able to go home from the hospital sooner when they had OMT.
In one small study, people with Parkinson's disease were able to walk better after only one session of OMT. Another study looked at 38 patients who had knee surgery. Those who had OMT were able to walk up stairs 20% earlier than those who did not have OMT.
A study of 100 people with high blood pressure treated only with OMT showed that OMT produced significant reductions in blood pressure.
Studies show that OMT eases breathing, drains the sinuses and relieves the symptoms, duration, and recurrence of the common cold.
Osteopathy may also be an effective way to treat carpal tunnel syndrome. More studies are needed to confirm this.
Examples of other conditions for which OMT may be helpful include:
stress-related problems (such as tension headaches, muscle spasm)
strains and sprains (especially of the neck and back)
shoulder pain
osteoarthritis
headaches
painful menstruation
injuries (such as whiplash)
scoliosis (side to side curvature of the spine)
infantile colic
insomnia
Osteopathic study: Treatment cuts pain
Source: PCOM News Release
The Philadelphia College of Osteopathic Medicine has produced what it is calling the first study that provides "objective data" demonstrating how osteopathic manipulative treatment, or OMT, can reduce pain after surgery.
OMT focuses on learning the body's interconnected system of nerves, muscles and nerves, and understanding how an injury or illness to one part of the body can affect another. Doctors in osteopathic medical schools are taught how to use their hands to diagnose injuries and illness, and how to manipulate the musculoskeletal system to encourage the body's natural tendency to heal itself.
The PCOM study, led by Dr. Frederick Goldstein, involved 33 hysterectomy patients at City Avenue Hospital who were all unfamiliar with OMT.
Researchers measured the amount of morphine that was required to treat pain, and the patients' perception of the pain levels, following the surgical procedure.
The study contained two variables. Some patients received morphine prior to surgery and others received a saline solution. After surgery, certain patients from each group received OMT while the others got "sham OMT," where a doctor placed his or her hands on specific areas of the patients, but did not perform any manipulation.
The preliminary results of the study showed OMT had a greater effect than drugs in reducing post-operative pain, and that the osteopathic treatment worked to reduce pain regardless of whether the patients received morphine or saline prior to surgery.
"This study is breakthrough scientific proof that OMT has a crucial role in treating patients who are in pain," Goldstein said.
Goldstein and his team plan to release additional study results within the next six months.
Tuesday, December 27, 2005
STRAIN AND COUNTERSTRAIN TECHNIQUE
Source: www.indianaholistichealth.net/glossary.htm
This is a very gentle form of treatment that can be used on almost any patient. The basis of this technique is the location of tender points, which are painful areas in myofascial structures that do not radiate to other parts of the body.
DEFINITION
Considered an INDIRECT method if treatment in which the dysfunctional tissue is positioned at a point of ease, or balance, which is away from the restrictive barrier. It is based upon identifying tender points and positioning the patient so that the tenderness is relieved. Strain/counterstrain was discovered in 1955 by Lawrence H. Jones, D.O. This technique was originally called spontaneous release by positioning and has also been called positional release therapy (frequently by physical therapists).
PRINCIPLES OF TREATMENT
This is a very gentle form of treatment that can be used on almost any patient. The basis of this technique is the location of tender points, which are painful areas in myofascial structures that do not radiate to other parts of the body.
DEFINITION
Considered an INDIRECT method if treatment in which the dysfunctional tissue is positioned at a point of ease, or balance, which is away from the restrictive barrier. It is based upon identifying tender points and positioning the patient so that the tenderness is relieved. Strain/counterstrain was discovered in 1955 by Lawrence H. Jones, D.O. This technique was originally called spontaneous release by positioning and has also been called positional release therapy (frequently by physical therapists).
PRINCIPLES OF TREATMENT
- Locate the significant tender point.
- Place the patient in a position of optimal comfort. The goal for pain reduction should be at least 70%.
- Maintain the position of comfort for 90 seconds (120 seconds for ribs).
- Slowly return the patient to the starting position.
- Recheck the tender point.
Principles of the Cranial Techniques
Source: pages.prodigy.net/stn1/Cranial%20Technique.htm
William Garner Sutherland, D.O., was the founder of cranial technique. He first began to theorize movement of the cranial bones in 1899 while a student at the American School of Osteopathy in Kirksville, Missouri. Upon graduation in the class of 1900, he devoted 30 years of research and study on the subject before he began presenting the concept to the osteopathic profession. After many lectures and presentations, he published The Cranial Bowl in 1939. In 1947 the Osteopathic Cranial Association was formed as an affiliate of the Academy of Applied Osteopathy, and the Sutherland Cranial Teaching Foundation was established in 1953.
PRINCIPLES OF CRANIAL TECHNIQUE
THE PRIMARY RESPIRATORY MECHANISM (PRM)
Primary- Underlying all other physiologic functions.
Respiratory- Concerned with cellular respiration.
Mechanism- Cranial articulations.
The PRM is often described in terms of the rhythm of the cranium, called the cranial rhythmic impulse (CRI). The rate of the CRI is from 6-12 to 10-14 cycles per minute, depending on what source you read. The central focus of this mechanism is the SPHENOBASILAR SYMPHYSIS (SBS). This is also referred to as the sphenobasilar synchondrosis or the sphenobasilar junction.
The components of the primary respiratory mechanism are as follows:
The anatomy of the cranial bones and their design for motion.
The mobility of the dural membranes (reciprocal tension membrane).
The inherent mobility of the brain and spinal cord, a constant rhythm of discharge and recharge of cells accompanied by a change in cell size.
The fluctuation of the cerebral spinal fluid.
The articular mobility of the sacrum between the ilia.
THE RECIPROCAL TENSION MEMBRANE (RTM)
Dr. Sutherland hypothesized that the motion of the cranial bones originated from the sphenoid and that the DRIVING FORCE for the sphenoid came from the rhythmic fluctuation of the CSF, which was harnessed and transferred to the sphenoid through the dural membrane system. Think of the RTM as the guiding and limiting mechanism for the cranial and sacral bones as they are involved in the PRM. The axis around which the membranes move is called the SUTHERLAND FULCRUM in his honor. This fulcrum is the point along which all tension in the dural membranes is focused. It is located where the falx cerebri and the two parts of the tentorium cerebelli meet (in the area of the straight sinus).
Components of the reciprocal tension membrane:
1. Falx cerebri.
2. Falx cerebelli
3. Tentorium cerebelli
4. Spinal dura
William Garner Sutherland, D.O., was the founder of cranial technique. He first began to theorize movement of the cranial bones in 1899 while a student at the American School of Osteopathy in Kirksville, Missouri. Upon graduation in the class of 1900, he devoted 30 years of research and study on the subject before he began presenting the concept to the osteopathic profession. After many lectures and presentations, he published The Cranial Bowl in 1939. In 1947 the Osteopathic Cranial Association was formed as an affiliate of the Academy of Applied Osteopathy, and the Sutherland Cranial Teaching Foundation was established in 1953.
PRINCIPLES OF CRANIAL TECHNIQUE
THE PRIMARY RESPIRATORY MECHANISM (PRM)
Primary- Underlying all other physiologic functions.
Respiratory- Concerned with cellular respiration.
Mechanism- Cranial articulations.
The PRM is often described in terms of the rhythm of the cranium, called the cranial rhythmic impulse (CRI). The rate of the CRI is from 6-12 to 10-14 cycles per minute, depending on what source you read. The central focus of this mechanism is the SPHENOBASILAR SYMPHYSIS (SBS). This is also referred to as the sphenobasilar synchondrosis or the sphenobasilar junction.
The components of the primary respiratory mechanism are as follows:
The anatomy of the cranial bones and their design for motion.
The mobility of the dural membranes (reciprocal tension membrane).
The inherent mobility of the brain and spinal cord, a constant rhythm of discharge and recharge of cells accompanied by a change in cell size.
The fluctuation of the cerebral spinal fluid.
The articular mobility of the sacrum between the ilia.
THE RECIPROCAL TENSION MEMBRANE (RTM)
Dr. Sutherland hypothesized that the motion of the cranial bones originated from the sphenoid and that the DRIVING FORCE for the sphenoid came from the rhythmic fluctuation of the CSF, which was harnessed and transferred to the sphenoid through the dural membrane system. Think of the RTM as the guiding and limiting mechanism for the cranial and sacral bones as they are involved in the PRM. The axis around which the membranes move is called the SUTHERLAND FULCRUM in his honor. This fulcrum is the point along which all tension in the dural membranes is focused. It is located where the falx cerebri and the two parts of the tentorium cerebelli meet (in the area of the straight sinus).
Components of the reciprocal tension membrane:
1. Falx cerebri.
2. Falx cerebelli
3. Tentorium cerebelli
4. Spinal dura
Saturday, December 24, 2005
Knee Cap Degeneration and the benefits of Osteopathic Manipulative Treatment
Source: www.joselitodelacruz.com/Knee_pain.htm
Knee Cap Degeneration
(wearing down of the lining under the knee cap)
Causes:
Frequent falls compressing the knee cap against the underlying bone, causing wear and tear of the cartilage lining.
Shortening of one side of the knee muscles, causing misalignment of the knee cap.
Dropped foot arch causing a twist in the knee and misaligning the knee cap.
Excessive twisting of the hips straining the knee.
Compensatory strain of the knee from lower back injuries or limping from foot problems.
Treatment:
A complete mechanical analysis of the knee and other joints. Balancing ligaments that are strained with local deep friction and ultrasound therapy to reduce inflammation and promote recovery. Muscular stretching to shortened muscles and deep soft tissue release to muscles that have adhesions combined with muscle energy techniques to rebalance muscle co-ordination. Craniosacral treatments to release and improve previously sustained stress and strains.
Where DOs can help: Osteopaths are quite good at analysing knee problems because we take into consideration mechanical problems elsewhere in the body that have direct and indirect connections with the knee. We also work with podiatrists (foot specialists) when further analysis is required for foot related problems
Knee Cap Degeneration
(wearing down of the lining under the knee cap)
Causes:
Frequent falls compressing the knee cap against the underlying bone, causing wear and tear of the cartilage lining.
Shortening of one side of the knee muscles, causing misalignment of the knee cap.
Dropped foot arch causing a twist in the knee and misaligning the knee cap.
Excessive twisting of the hips straining the knee.
Compensatory strain of the knee from lower back injuries or limping from foot problems.
Treatment:
A complete mechanical analysis of the knee and other joints. Balancing ligaments that are strained with local deep friction and ultrasound therapy to reduce inflammation and promote recovery. Muscular stretching to shortened muscles and deep soft tissue release to muscles that have adhesions combined with muscle energy techniques to rebalance muscle co-ordination. Craniosacral treatments to release and improve previously sustained stress and strains.
Where DOs can help: Osteopaths are quite good at analysing knee problems because we take into consideration mechanical problems elsewhere in the body that have direct and indirect connections with the knee. We also work with podiatrists (foot specialists) when further analysis is required for foot related problems
Aims of Osteopathic Diagnosis
Source: www.osteopathic.org/index.cfm?PageID=ost_tenet
The aims of osteopathic diagnosis are two fold:
The aims of osteopathic diagnosis are two fold:
- To identify the site of the source of the symptoms and the nature of the tissue disturbance.
- To assess the mechanical structure and function of the body.
It is the second aim that differentiates the osteopathic approach, both in the evaluation of the patient and consequently in treatment. It emphasizes not only of the local tissue damage or disturbance but also the interaction with the rest of the body. This is a two way process; the local dysfunction has an impact on the rest of the body but equally the local response will be affected by factors in other parts. It is our ultimately our purpose to assist the person to cope with and where possible, overcome the problem so long as it is amenable to an osteopathic approach. Osteopathic musculoskeletal evaluation is unique in that palpation is integrated with motion testing. Osteopathy emphasizes the interrelationships between structure (anatomy) and function (physiology).
But the osteopathic profession sees itself as being relevant to a wide range of health problems, and not simply limited to the treatment of musculoskeletal derangements. Osteopathic theory and practice are firmly in line with the concepts of Hippocrates. The patient is considered and treated as a whole. Founded as it was in this tradition, osteopathy is patient orientated rather than disease orientated. It has utilized structural diagnosis and manipulative treatment as part of its philosophy and practice, and therefore as part of total patient care, not confining it to painful conditions of the musculoskeletal systems alone.
According to the AOA, here are the tenets of osteopathic medicine:
http://www.osteopathic.org/index.cfm?PageID=ost_tenet
Tenets of Osteopathic Medicine
First, do no harm. A thoughtful diagnosis should be made before exposing the patient to any potentially harmful procedure.
Look beyond the disease for the cause. Treatment should center on the cause, with effect addressed only when it benefits the patient in some tangible way.
The practice of medicine should be based on sound medical principles. Only therapies proven clinically beneficial in improving patient outcome should be recommended.
The body is subject to mechanical laws. The science of physics applies to humans. Even a slight alteration in the body’s precision can result in disorders that overcome natural defenses.
The body has the potential to make all substances necessary to insure its health. No medical approach can exceed the efficacy of the body’s natural defense systems if those defenses are functioning properly. Therefore, teaching the patient to care for his own health and to prevent disease is part of a physician’s responsibility.
The nervous system controls, influences, and/or integrates all bodily functions.
Osteopathy embraces all known areas of practice.
Osteopathic Treatment of Neck Problems
Source: www.backandbodycare.com/home/neck/neck.htm
Joint strain/lock
Osteopaths are able to feel and locate locked joints that are causing the pain.
Cause: Sports injuries, keeping the neck turned for too long, sleeping with high/low pillows, turning too quickly.
Treatment: Osteopathic manipulation to release the joints, mobilisation to increase the range of movement. Ultrasound therapy may be used. Balancing the ligaments that hold joints together.
Background: Manipulation of locked joints frees the neck and improves the range.
Clicking of these joints is not the same as when people click their own neck; they are not as specific and tend to click the same joints for years, causing future problems.
With osteopathic treatment and management people click their neck less often, feel more flexibility. They can turn their head further and have less discomfort.
Massage often helps temporarily to release the muscles, but without releasing the locked joint the stiffness soon returns. However, osteopathic deep soft massage can give longer relief because muscles are also stretched and lengthened to allow the joints to move freely. Otherwise residual stiffness can remain for a long time.
Upper Rib Problems
People are often surprised when they are told that the cause of their neck pain or stiffness is due to their ribs.
Cause: Sleeping on one side for too long with wrong pillow height, previous unresolved injury, muscle- or joint-trauma, compression from a spinal curvature.
Treatment: Deep soft tissue release of the muscles in between ribs as well as increasing the gap between rib segments, manipulation of the rib joints in the spine. Balancing the ligaments that hold joints together.
Background: Individual ribs can be injured and cause discomfort during breathing and neck movements. Upper rib problems tend to be painful on either side of the neck, between the shoulder blades and a few inches away from the spine. The pain is not sharp but often nagging and persistent. The discomfort can be quite deep, non-specific, and can vary.
People often ignore these symptoms until other overlapping problems become prominent.
Osteopaths examine other areas looking for structures that can contribute to the problem. This approach is different from orthopaedic surgeons or physiotherapists.
Osteopathic evaluation for neck complaints includes the examination of other structures like shoulders, mid back and rib cage. The examination can highlight long-standing upper rib pain that has intermittently caused discomfort for many years.
However, it is only after the detailed examination that patients realize the extent of their pain and the memory of the forgotten discomfort that they have come to accept.
The initial osteopathic treatment can relieve the current muscle and joint stiffness, but treating the underlying rib problems will provide long-term relief.
Scoliosis/curvature
There is a misconception that taking the “curve” out of the spine will relieve pain and discomfort. People with a straight spine also get back pain!
Cause: For some, the curvature runs in the family as a hereditary problem, for others poor posture and bad habits in the long term can promote a curvature. Long or short leg syndrome is a common cause.
Treatment: X-rays are often recommended to assess the curve in detail. Soft tissue stretching and joint/spinal manipulation are needed to allow the body to compensate better for the curvature. Craniosacral techniques to release the internal stress and strains of the body.
Background: Osteopathic principles guide osteopaths to improve mobility, flexibility and function of the body and not just the spine, allowing the body to cope better under any circumstance - this includes scoliosis.
Scoliosis is not a disease but a description of the curvature of the spine. No person is 100% symmetrical and everyone is dominant on one side (the majority are right hand dominant). And so everyone has some form of curvature, which varies within a given range.
Patients with neck pain/stiffness resulting from a curvature in the mid back can get pain relief by osteopathic manipulation and mobilization of the soft tissues (muscles, ligaments, tendons) and joints.
The aim is to release any restriction around the mid back and neck to give the body a chance to compensate better for the curvature.
These treatments result in reducing both the constant daily stiffness and the frequency of clicking their own neck and an improved posture.
Trapped Nerves
Tingling and numbness in the hand and fingers constitute compression of spinal nerves at the lower part of the neck.
Cause: Compression and damage to discs (spondylosis), shortened and very tight muscles in the front and side of the neck can compress the nerves and blood vessels of the arm
Treatment: Patients can get relief from osteopathic manipulation - not simply applying traction to the neck, which is the standard hospital treatment, but by local and general treatment to the upper girdle (shoulder and head/neck) and lower girdle (pelvis and hips). Craniosacral techniques to release tension in the upper girdle and resolve previous trauma.
Background: Osteopathic manipulation can reduce the amount of hand symptoms for a person suffering from spondylosis.
There is no cure for this condition but rather a better treatment regime. They will always be prone to recurring symptoms, which is why exercise and posture correction are prescribed.
Treatment reduces the compression of the nerves, and osteopathic examination identifies factors that contribute to the nerve irritation.
These can be from poor posture, bad sleeping habits, lack of exercise or unresolved joint problems.
Pre-Surgery
Osteopathic treatment can help prepare the structures around the neck prior to surgery. This will help to improve the recovery rate.
Post-Surgery
Disc operations in the neck are un-common but for those who have undergone this procedure, osteopathic treatment can often provide relief from neck stiffness, nerve compression, joint degeneration and muscle tightness.
First Aid to Neck problems
Use ice compress as soon as possible for 10 minutes to reduce inflammation. Take a break for 10 minutes and repeat 3x. This can be done every 2-3 hours for the first 1-2 days.
Take some anti-inflammatory tablets to control pain and reduce inflammation. Take care if you have sensitive stomach lining or ulcers.
If the pain is severe, make an appointment with the osteopath
If the pain persists after two days, see the osteopath. Take note that your body takes longer to recover if you delay your treatment.
If in doubt, call the osteopath for advice.
Find a DO near you today!
Joint strain/lock
Osteopaths are able to feel and locate locked joints that are causing the pain.
Cause: Sports injuries, keeping the neck turned for too long, sleeping with high/low pillows, turning too quickly.
Treatment: Osteopathic manipulation to release the joints, mobilisation to increase the range of movement. Ultrasound therapy may be used. Balancing the ligaments that hold joints together.
Background: Manipulation of locked joints frees the neck and improves the range.
Clicking of these joints is not the same as when people click their own neck; they are not as specific and tend to click the same joints for years, causing future problems.
With osteopathic treatment and management people click their neck less often, feel more flexibility. They can turn their head further and have less discomfort.
Massage often helps temporarily to release the muscles, but without releasing the locked joint the stiffness soon returns. However, osteopathic deep soft massage can give longer relief because muscles are also stretched and lengthened to allow the joints to move freely. Otherwise residual stiffness can remain for a long time.
Upper Rib Problems
People are often surprised when they are told that the cause of their neck pain or stiffness is due to their ribs.
Cause: Sleeping on one side for too long with wrong pillow height, previous unresolved injury, muscle- or joint-trauma, compression from a spinal curvature.
Treatment: Deep soft tissue release of the muscles in between ribs as well as increasing the gap between rib segments, manipulation of the rib joints in the spine. Balancing the ligaments that hold joints together.
Background: Individual ribs can be injured and cause discomfort during breathing and neck movements. Upper rib problems tend to be painful on either side of the neck, between the shoulder blades and a few inches away from the spine. The pain is not sharp but often nagging and persistent. The discomfort can be quite deep, non-specific, and can vary.
People often ignore these symptoms until other overlapping problems become prominent.
Osteopaths examine other areas looking for structures that can contribute to the problem. This approach is different from orthopaedic surgeons or physiotherapists.
Osteopathic evaluation for neck complaints includes the examination of other structures like shoulders, mid back and rib cage. The examination can highlight long-standing upper rib pain that has intermittently caused discomfort for many years.
However, it is only after the detailed examination that patients realize the extent of their pain and the memory of the forgotten discomfort that they have come to accept.
The initial osteopathic treatment can relieve the current muscle and joint stiffness, but treating the underlying rib problems will provide long-term relief.
Scoliosis/curvature
There is a misconception that taking the “curve” out of the spine will relieve pain and discomfort. People with a straight spine also get back pain!
Cause: For some, the curvature runs in the family as a hereditary problem, for others poor posture and bad habits in the long term can promote a curvature. Long or short leg syndrome is a common cause.
Treatment: X-rays are often recommended to assess the curve in detail. Soft tissue stretching and joint/spinal manipulation are needed to allow the body to compensate better for the curvature. Craniosacral techniques to release the internal stress and strains of the body.
Background: Osteopathic principles guide osteopaths to improve mobility, flexibility and function of the body and not just the spine, allowing the body to cope better under any circumstance - this includes scoliosis.
Scoliosis is not a disease but a description of the curvature of the spine. No person is 100% symmetrical and everyone is dominant on one side (the majority are right hand dominant). And so everyone has some form of curvature, which varies within a given range.
Patients with neck pain/stiffness resulting from a curvature in the mid back can get pain relief by osteopathic manipulation and mobilization of the soft tissues (muscles, ligaments, tendons) and joints.
The aim is to release any restriction around the mid back and neck to give the body a chance to compensate better for the curvature.
These treatments result in reducing both the constant daily stiffness and the frequency of clicking their own neck and an improved posture.
Trapped Nerves
Tingling and numbness in the hand and fingers constitute compression of spinal nerves at the lower part of the neck.
Cause: Compression and damage to discs (spondylosis), shortened and very tight muscles in the front and side of the neck can compress the nerves and blood vessels of the arm
Treatment: Patients can get relief from osteopathic manipulation - not simply applying traction to the neck, which is the standard hospital treatment, but by local and general treatment to the upper girdle (shoulder and head/neck) and lower girdle (pelvis and hips). Craniosacral techniques to release tension in the upper girdle and resolve previous trauma.
Background: Osteopathic manipulation can reduce the amount of hand symptoms for a person suffering from spondylosis.
There is no cure for this condition but rather a better treatment regime. They will always be prone to recurring symptoms, which is why exercise and posture correction are prescribed.
Treatment reduces the compression of the nerves, and osteopathic examination identifies factors that contribute to the nerve irritation.
These can be from poor posture, bad sleeping habits, lack of exercise or unresolved joint problems.
Pre-Surgery
Osteopathic treatment can help prepare the structures around the neck prior to surgery. This will help to improve the recovery rate.
Post-Surgery
Disc operations in the neck are un-common but for those who have undergone this procedure, osteopathic treatment can often provide relief from neck stiffness, nerve compression, joint degeneration and muscle tightness.
First Aid to Neck problems
Use ice compress as soon as possible for 10 minutes to reduce inflammation. Take a break for 10 minutes and repeat 3x. This can be done every 2-3 hours for the first 1-2 days.
Take some anti-inflammatory tablets to control pain and reduce inflammation. Take care if you have sensitive stomach lining or ulcers.
If the pain is severe, make an appointment with the osteopath
If the pain persists after two days, see the osteopath. Take note that your body takes longer to recover if you delay your treatment.
If in doubt, call the osteopath for advice.
Find a DO near you today!
Osteopathic Manipulative Treatment-Some common questions by patients
Source: www.healthywomen.org/content. cfm?L1=3&L2=102&L3=6.0000
My doctor of osteopathic medicine (DO) didn't perform osteopathic manipulative treatment (OMT) on me. Why?
DOs will select the best therapy or other modalities that are necessary for the treatment of the patient as a whole. Not all conditions or each visit will require OMT. Remember, DOs are indistinguishable from medical doctors (MD) and thus utilize the standards of treatment, but are afforded an extra modality of OMT when appropriate.
I had a few sessions of osteopathic manipulative treatment (OMT) and I don't feel any better.
Manipulation takes time as well as your participation in maintaining your treatment by making postural changes and other life style changes in order for your condition to improve. Talk to your DO about other approaches to maintaining your treatment.
How does osteopathic medicine differ from chiropractics?
The most obvious distinction is that chiropractors are not the legal equivalents of MDs—they can't prescribe medication or perform surgery. Although both DOs and chiropractors practice manipulation and share a philosophy that good health is tied to the body's structure, chiropractors focus almost exclusively on realigning the bones and joints. DOs also practice traditional medicine and can treat a range of conditions with an array of tools.
A friend of mine had craniosacral therapy. Is that the same thing as cranial osteopathic medicine?
No. Cranial sacral osteopathic medicine is practiced by trained DOs (and some MDs); it involves gentle pressure to your head in a directed manner to obtain desired results. Craniosacral therapy is usually practiced by physical therapists, massage therapists or other alternative health professionals who never attended medical school. It may have its benefits, but it has its limitations in that it is not the complete treatment of the cranial sacral regions of the body. Be sure to talk to your health care professional before pursuing it.
My doctor of osteopathic medicine (DO) didn't perform osteopathic manipulative treatment (OMT) on me. Why?
DOs will select the best therapy or other modalities that are necessary for the treatment of the patient as a whole. Not all conditions or each visit will require OMT. Remember, DOs are indistinguishable from medical doctors (MD) and thus utilize the standards of treatment, but are afforded an extra modality of OMT when appropriate.
I had a few sessions of osteopathic manipulative treatment (OMT) and I don't feel any better.
Manipulation takes time as well as your participation in maintaining your treatment by making postural changes and other life style changes in order for your condition to improve. Talk to your DO about other approaches to maintaining your treatment.
How does osteopathic medicine differ from chiropractics?
The most obvious distinction is that chiropractors are not the legal equivalents of MDs—they can't prescribe medication or perform surgery. Although both DOs and chiropractors practice manipulation and share a philosophy that good health is tied to the body's structure, chiropractors focus almost exclusively on realigning the bones and joints. DOs also practice traditional medicine and can treat a range of conditions with an array of tools.
A friend of mine had craniosacral therapy. Is that the same thing as cranial osteopathic medicine?
No. Cranial sacral osteopathic medicine is practiced by trained DOs (and some MDs); it involves gentle pressure to your head in a directed manner to obtain desired results. Craniosacral therapy is usually practiced by physical therapists, massage therapists or other alternative health professionals who never attended medical school. It may have its benefits, but it has its limitations in that it is not the complete treatment of the cranial sacral regions of the body. Be sure to talk to your health care professional before pursuing it.
Friday, December 23, 2005
Curing Headaches and Migraine
Source: www.indiangyan.com/books/therapybooks/ Osteopathy/Headaches_Migraine.shtml
A headache is a common problem today. Who does not get a headache? An executive, a philosopher, a scientist, a business magnate, a clerk, a housewife, a student - everybody, at sometime or other, is afflicted by a headache! It has no professional or age barriers.
Women suffer more than men. The reason may well be pre-menstrual migraines during puberty. These get worse as the years roll by, and are cured only by menopause. Contraceptives are known to cause headaches in some women and cure them in others. Headaches may become less frequent in pregnancy. In fact, a headache is not a killing disease, but its attack is so intense that all the nerves in the skull start throbbing due to great pressure.
A lot of research has been done to find out the cause of headaches.
What is a headache? Is it an allergic disease caused by something we eat or breathe? Has it any relation to our posture, incorrect way of sitting, standing or working? Is it a product of tension in our day-to-day life, a way to relieve frustration? Or is it due to some mechanical problem in the neck or head itself?
In the 5th century, it was thought that a headache was due to a severe chill, exposure to sunlight, or even fatigue. In the 11th century, it was thought that it occurred after having cold things in our food. According to Tissort (1784), vomiting often concluded an attack. He also suggested that a reflex irritation of the gastric nerves resulted in an attack of migraine. Living (1873) said that a headache was related to asthma and a convulsive state. Rilay (1932) suggested that it occurred when noxious vapor entered the cerebral blood vessels. According to another opinion, it occurred due to eye strain. A few researchers concluded that it was due to adhesions of the cerebral membranes and formation of excessive cerebro-spinal fluid. Disorders of the ovaries and thyroid were also thought to cause migraines. Emotional problems were also attributed to headaches - for instance, a difficult father-and-son relationship in business, tough competition, a tense situation in the family, a hard struggle to get oneself established .... Apart from this, certain foods were found to cause headaches: chocolate, cheese, fruits, alcohol, fatty fried foods, tea, coffee, sea food, pork and many more.
Remedies
The long series of researches in this direction have shown that the human race has suffered a lot from headaches and though thousands of remedies have been prescribed, they have only succeeded in providing temporary relief Many migraine clinics and foundations have spent millions of rupees to find a remedy which will bring permanent relief These efforts are akin to ploughing in the sand! How long have we to live with such strong medications which produce side-effects in other systems of our body? After using a particular medicine for a long time, it loses its effectiveness anyway.
Sometimes, while suffering from a headache, a striking idea, solution or news gets rid of the headache and the patient becomes normal again. During a battle, General Ulysses S. Grant was seized with an attack of migraine. The limping general received the good news that his enemy was ready to surrender. Ulysses sprang to his feet at this glad news, and his headache vanished miraculously.
Many victims change their environment, take to the Himalayas, Tibet or Somaliland, go from the highest altitude to the lowest, from the wettest to the driest, experiencing a new climate, food and cultural changes but the migraine remains, because they carry their personal environment with them.
Headache of Cervical Origin
Frequently, a chronic headache resistant to treatment is due to a disorder of the cervical spine, which may be cured by manipulation. Certain mechanical changes in the cervical spine may cause an intermittent or a continuous headache. These changes respond well to manipulation. The pain can spring from the neck. Some people do not believe in the possibility that pain can radiate from the neck to the head.
An experiment was carried out by Kellgreen. A concentrated saline solution was injected in the area where the cervical spine first joins with the head, producing tenderness and headache in the forehead region. This proved a connection between the neck and the forehead.
Important changes have been found in the cervical spine in cases of headaches. These relate to disturbances in the lumen of the vertebral artery which passes through the transverse process of the cervical vertebrae and supplies blood to the brain.
Sometimes the therapeutic effect of cervical manipulation helps us to confirm whether a particular headache is of cervical origin.
Sometimes a headache is produced by the head being kept in a certain position; keeping it in the opposite direction relieves the headache. Sometimes manual traction at the neck relieves the headache. These are indications that headaches may be of cervical origin, and manipulation succeeds.
Embryological, the head and the first and second cervical vertebrae are formed by the first and second cervical segment.
As they originate from the same segments they ought to have some relationship between them. So any abnormality at the level of the first and second cervical vertebrae can give rise to pain in any part of the head, the temple and the forehead. As it happens elsewhere, local pain at the level of the cervical vertebrae may be completely absent and the patient may complain only of a headache.
This type of headache may come on while waking up in the morning. It may be felt in the back of the head or the front of the head, or may be only in the forehead. This begins to ease after some hours and is much better by mid-day. The patient is free from headache till the next morning. As the years pass by, the headache may tend to last longer during the day. It responds well to manipulative treatment.
Dr Bicker's staff is of the opinion that headache is due to stretching or tension in the muscles, vessels or the outermost sheath of the spinal chord. If it is due to these mechanical reasons, the pain starts in the upper neck muscles, and spreads to the upper back and head. Instead of being limited in this area, it spreads to the entire head. It may be associated with stiffness and pain in the upper neck. It occurs off and on. The -headache seems to spread from the neck to the head rather than from the head to the neck.
There can be other causes of headaches too. Keeping that in mind, a detailed history of the patient can help in pinpointing the cause of the headache.
At times differentiation is difficult. But distinction is important, as headaches arising from the neck can most easily and lastingly be relieved'. So it is a great pity when the right diagnosis is not made and the right treatment is not administered. Am old man is often told that his headache is due to high blood pressure. In fact, it may be completely unconnected and it may be due to upper cervical osteoarthritis. Cervical manipulation can relieve pain on the lateral side of the face. This pain often has rhythmically and may be associated with a running nose or watering of the eyes. It may radiate to the upper jaw or even the lower jaw. The patient is often referred to a dental surgeon or oral surgeon.
Osteopathic examination may show tenderness over the side of the second and third cervical vertebra on the same side, and if the X-ray picture is clear, manipulation will be successful in many cases and the pain will subside.
Other Possible Causes of Headaches
• Eye strain due to defective eyesight
• Sinusitis
• Toothache
• Digestive disturbances
• Neurological problems, e.g., an intra-cranial tumour
• Allergy
• Cardiovascular diseases
• Psychogenic (mental) frustration
Upper cervical pain may be caused by:
An intra-cranial tumour of the posterior fossa (portion) of the skull.
A disease of the upper cervical spine such as tuberculosis,
Malignancy
Migraine
Headaches occurring at intervals on the right or left side of the head, are associated with nausea and vomiting. There may be a feeling of seeing non-existent objects in front of the eyes before the onset of the headache. Such headaches usually start before the age of 30.
Many such patients respond to manipulation. In some cases Migraine may occur at the back of the head. In such cases manipulation will relieve the headache to a considerable degree.
Migraine of Cervical Origin.
Spondylosis and osteo-arthritic changes in the cervical spine can cause an inflammatory reaction. This causes a spasm in the vertebral artery and its branches, resulting in a headache with the following characteristics:
1. It is mostly localized in the forehead and may be associated with nausea and severe vomiting. The headache always occurs on the same side. Manipulation elicits a good response.
2. Sometimes the headache is localized at the back of the eyeball and the initial symptoms pertain to visual abnormalities.
Case Histories
A girl, eleven years old, had a severe headache for five days. She underwent laboratory tests of blood, urine, and stool. X-rays were also taken. Every finding was normal and the cause could not be detected. In spite of all possible medication she did not show any improvement. She was thought to be a case fit for a psychiatrist. But her father brought the child to me and narrated the following history: she complained of upper back pain when she went to school with a heavy bag strapped across her shoulders. This pain continued till late evening. She became irritable and would not listen to her parents.
The history of irritability and failure of drugs proved that her ailment was not physical but mental. She was treated manipulatively three times and her headache completely disappeared. She was taught to walk straight instead of going about with a forward stoop. She showed complete recovery.
A 29-year-old lady with three children had been getting headaches off and on since her college days. She also suffered from severe pain in the neck and both shoulders. The headache would occur twice or thrice a month during the day, lasting each time for 10-20 minutes. It would become less during the menstruation cycles. After she got married, the headaches went on increasing in frequency and intensity, and for two years she got headaches every day and had to resort to pain killers. The headaches were accompanied by tension in the neck and were more intense at the back of the head and in the frontal area, in her eyeballs and behind them.
Her condition was diagnosed as migraine. She was given manipulative treatment for her cervical spine and upper dorsal spine. Gradually the headaches started getting less frequent and less intense. She rarely used a pain killer. In 10 weeks the headaches completely subsided.
A 36-year-old engineer employed in the Railways had been suffering from headaches since his school days. They used to occur at fortnightly intervals and later, almost every week. The pain was very severe, starting from the back of the head and then spreading all over the head. He also felt pain in the upper back. His veins became prominent in the temples during the attack, and throbbed. He suffered from nausea and vomiting and would turn away from food or drink. All this would last for twenty-four hours, sometimes even for two to three days. Occasionally, when there was no severe headache, there would be a feeling of general uneasiness. He would prefer to remain in the dark and not be disturbed. He also preferred to lie down till recovery. He was given glasses as his sight was found to be weak, but this did not help. He consulted many doctors and took treatment, but to no avail.
He came to me with his complaint. I examined him thoroughly and found him to have a round upper back. X-rays of the cervical and dorsal spine were taken, but they did not reveal any abnormality; other pathological tests too were all normal.
Manipulative treatment was started. He felt no improvement after the first session. He was called again after a week and manipulative treatment of the cervical and dorsal spine was repeated. He felt some improvement. After a few weeks, his headache became less severe and less frequent. In three months he felt completely recovered, but he continued to come once a month for three months. He has since been advised to come twice a year for maintenance treatment. He has had no attacks ever since.
A young girl aged 21 years suffered from headaches for eight years. At first, she used to have a headache once a month or once a fortnight. During the last three years, the headaches became more frequent and she started having headaches almost every day. The ache was in the entire head, though more severe in the forehead. She did not get nausea or vomiting. Due to the severity of the headaches, she had to discontinue her studies. She was examined by a few doctors but nothing seemed to help her.
She was then referred to me for manipulative treatment. After being treated for three weeks, she felt much better. By the end of six weeks, she was completely cured and the headaches never returned. She has resumed her studies happily.
A good website for more information:
http://www.headaches.org/
A headache is a common problem today. Who does not get a headache? An executive, a philosopher, a scientist, a business magnate, a clerk, a housewife, a student - everybody, at sometime or other, is afflicted by a headache! It has no professional or age barriers.
Women suffer more than men. The reason may well be pre-menstrual migraines during puberty. These get worse as the years roll by, and are cured only by menopause. Contraceptives are known to cause headaches in some women and cure them in others. Headaches may become less frequent in pregnancy. In fact, a headache is not a killing disease, but its attack is so intense that all the nerves in the skull start throbbing due to great pressure.
A lot of research has been done to find out the cause of headaches.
What is a headache? Is it an allergic disease caused by something we eat or breathe? Has it any relation to our posture, incorrect way of sitting, standing or working? Is it a product of tension in our day-to-day life, a way to relieve frustration? Or is it due to some mechanical problem in the neck or head itself?
In the 5th century, it was thought that a headache was due to a severe chill, exposure to sunlight, or even fatigue. In the 11th century, it was thought that it occurred after having cold things in our food. According to Tissort (1784), vomiting often concluded an attack. He also suggested that a reflex irritation of the gastric nerves resulted in an attack of migraine. Living (1873) said that a headache was related to asthma and a convulsive state. Rilay (1932) suggested that it occurred when noxious vapor entered the cerebral blood vessels. According to another opinion, it occurred due to eye strain. A few researchers concluded that it was due to adhesions of the cerebral membranes and formation of excessive cerebro-spinal fluid. Disorders of the ovaries and thyroid were also thought to cause migraines. Emotional problems were also attributed to headaches - for instance, a difficult father-and-son relationship in business, tough competition, a tense situation in the family, a hard struggle to get oneself established .... Apart from this, certain foods were found to cause headaches: chocolate, cheese, fruits, alcohol, fatty fried foods, tea, coffee, sea food, pork and many more.
Remedies
The long series of researches in this direction have shown that the human race has suffered a lot from headaches and though thousands of remedies have been prescribed, they have only succeeded in providing temporary relief Many migraine clinics and foundations have spent millions of rupees to find a remedy which will bring permanent relief These efforts are akin to ploughing in the sand! How long have we to live with such strong medications which produce side-effects in other systems of our body? After using a particular medicine for a long time, it loses its effectiveness anyway.
Sometimes, while suffering from a headache, a striking idea, solution or news gets rid of the headache and the patient becomes normal again. During a battle, General Ulysses S. Grant was seized with an attack of migraine. The limping general received the good news that his enemy was ready to surrender. Ulysses sprang to his feet at this glad news, and his headache vanished miraculously.
Many victims change their environment, take to the Himalayas, Tibet or Somaliland, go from the highest altitude to the lowest, from the wettest to the driest, experiencing a new climate, food and cultural changes but the migraine remains, because they carry their personal environment with them.
Headache of Cervical Origin
Frequently, a chronic headache resistant to treatment is due to a disorder of the cervical spine, which may be cured by manipulation. Certain mechanical changes in the cervical spine may cause an intermittent or a continuous headache. These changes respond well to manipulation. The pain can spring from the neck. Some people do not believe in the possibility that pain can radiate from the neck to the head.
An experiment was carried out by Kellgreen. A concentrated saline solution was injected in the area where the cervical spine first joins with the head, producing tenderness and headache in the forehead region. This proved a connection between the neck and the forehead.
Important changes have been found in the cervical spine in cases of headaches. These relate to disturbances in the lumen of the vertebral artery which passes through the transverse process of the cervical vertebrae and supplies blood to the brain.
Sometimes the therapeutic effect of cervical manipulation helps us to confirm whether a particular headache is of cervical origin.
Sometimes a headache is produced by the head being kept in a certain position; keeping it in the opposite direction relieves the headache. Sometimes manual traction at the neck relieves the headache. These are indications that headaches may be of cervical origin, and manipulation succeeds.
Embryological, the head and the first and second cervical vertebrae are formed by the first and second cervical segment.
As they originate from the same segments they ought to have some relationship between them. So any abnormality at the level of the first and second cervical vertebrae can give rise to pain in any part of the head, the temple and the forehead. As it happens elsewhere, local pain at the level of the cervical vertebrae may be completely absent and the patient may complain only of a headache.
This type of headache may come on while waking up in the morning. It may be felt in the back of the head or the front of the head, or may be only in the forehead. This begins to ease after some hours and is much better by mid-day. The patient is free from headache till the next morning. As the years pass by, the headache may tend to last longer during the day. It responds well to manipulative treatment.
Dr Bicker's staff is of the opinion that headache is due to stretching or tension in the muscles, vessels or the outermost sheath of the spinal chord. If it is due to these mechanical reasons, the pain starts in the upper neck muscles, and spreads to the upper back and head. Instead of being limited in this area, it spreads to the entire head. It may be associated with stiffness and pain in the upper neck. It occurs off and on. The -headache seems to spread from the neck to the head rather than from the head to the neck.
There can be other causes of headaches too. Keeping that in mind, a detailed history of the patient can help in pinpointing the cause of the headache.
At times differentiation is difficult. But distinction is important, as headaches arising from the neck can most easily and lastingly be relieved'. So it is a great pity when the right diagnosis is not made and the right treatment is not administered. Am old man is often told that his headache is due to high blood pressure. In fact, it may be completely unconnected and it may be due to upper cervical osteoarthritis. Cervical manipulation can relieve pain on the lateral side of the face. This pain often has rhythmically and may be associated with a running nose or watering of the eyes. It may radiate to the upper jaw or even the lower jaw. The patient is often referred to a dental surgeon or oral surgeon.
Osteopathic examination may show tenderness over the side of the second and third cervical vertebra on the same side, and if the X-ray picture is clear, manipulation will be successful in many cases and the pain will subside.
Other Possible Causes of Headaches
• Eye strain due to defective eyesight
• Sinusitis
• Toothache
• Digestive disturbances
• Neurological problems, e.g., an intra-cranial tumour
• Allergy
• Cardiovascular diseases
• Psychogenic (mental) frustration
Upper cervical pain may be caused by:
An intra-cranial tumour of the posterior fossa (portion) of the skull.
A disease of the upper cervical spine such as tuberculosis,
Malignancy
Migraine
Headaches occurring at intervals on the right or left side of the head, are associated with nausea and vomiting. There may be a feeling of seeing non-existent objects in front of the eyes before the onset of the headache. Such headaches usually start before the age of 30.
Many such patients respond to manipulation. In some cases Migraine may occur at the back of the head. In such cases manipulation will relieve the headache to a considerable degree.
Migraine of Cervical Origin.
Spondylosis and osteo-arthritic changes in the cervical spine can cause an inflammatory reaction. This causes a spasm in the vertebral artery and its branches, resulting in a headache with the following characteristics:
1. It is mostly localized in the forehead and may be associated with nausea and severe vomiting. The headache always occurs on the same side. Manipulation elicits a good response.
2. Sometimes the headache is localized at the back of the eyeball and the initial symptoms pertain to visual abnormalities.
Case Histories
A girl, eleven years old, had a severe headache for five days. She underwent laboratory tests of blood, urine, and stool. X-rays were also taken. Every finding was normal and the cause could not be detected. In spite of all possible medication she did not show any improvement. She was thought to be a case fit for a psychiatrist. But her father brought the child to me and narrated the following history: she complained of upper back pain when she went to school with a heavy bag strapped across her shoulders. This pain continued till late evening. She became irritable and would not listen to her parents.
The history of irritability and failure of drugs proved that her ailment was not physical but mental. She was treated manipulatively three times and her headache completely disappeared. She was taught to walk straight instead of going about with a forward stoop. She showed complete recovery.
A 29-year-old lady with three children had been getting headaches off and on since her college days. She also suffered from severe pain in the neck and both shoulders. The headache would occur twice or thrice a month during the day, lasting each time for 10-20 minutes. It would become less during the menstruation cycles. After she got married, the headaches went on increasing in frequency and intensity, and for two years she got headaches every day and had to resort to pain killers. The headaches were accompanied by tension in the neck and were more intense at the back of the head and in the frontal area, in her eyeballs and behind them.
Her condition was diagnosed as migraine. She was given manipulative treatment for her cervical spine and upper dorsal spine. Gradually the headaches started getting less frequent and less intense. She rarely used a pain killer. In 10 weeks the headaches completely subsided.
A 36-year-old engineer employed in the Railways had been suffering from headaches since his school days. They used to occur at fortnightly intervals and later, almost every week. The pain was very severe, starting from the back of the head and then spreading all over the head. He also felt pain in the upper back. His veins became prominent in the temples during the attack, and throbbed. He suffered from nausea and vomiting and would turn away from food or drink. All this would last for twenty-four hours, sometimes even for two to three days. Occasionally, when there was no severe headache, there would be a feeling of general uneasiness. He would prefer to remain in the dark and not be disturbed. He also preferred to lie down till recovery. He was given glasses as his sight was found to be weak, but this did not help. He consulted many doctors and took treatment, but to no avail.
He came to me with his complaint. I examined him thoroughly and found him to have a round upper back. X-rays of the cervical and dorsal spine were taken, but they did not reveal any abnormality; other pathological tests too were all normal.
Manipulative treatment was started. He felt no improvement after the first session. He was called again after a week and manipulative treatment of the cervical and dorsal spine was repeated. He felt some improvement. After a few weeks, his headache became less severe and less frequent. In three months he felt completely recovered, but he continued to come once a month for three months. He has since been advised to come twice a year for maintenance treatment. He has had no attacks ever since.
A young girl aged 21 years suffered from headaches for eight years. At first, she used to have a headache once a month or once a fortnight. During the last three years, the headaches became more frequent and she started having headaches almost every day. The ache was in the entire head, though more severe in the forehead. She did not get nausea or vomiting. Due to the severity of the headaches, she had to discontinue her studies. She was examined by a few doctors but nothing seemed to help her.
She was then referred to me for manipulative treatment. After being treated for three weeks, she felt much better. By the end of six weeks, she was completely cured and the headaches never returned. She has resumed her studies happily.
A good website for more information:
http://www.headaches.org/
Wednesday, December 21, 2005
Osteopathic Manipulative Treatment(OMT): Muscle Energy Technique (MET)
Source: www.healthy.net/scr/article.asp?ID=1650
Muscle Energy Technique (MET) is a further method of applying direct action to a restricted area. With MET, however, it is the patient's own forces which produce the manipulative effort. By placing a joint in a precise position, and calling on the patient to use a muscular effort in a particular direction, against a distinctly executed counter-force from the practitioner, it is frequently possible to achieve dramatic improvements in joint mobility. The skill in such a manouevre is in creating a balance of forces which can operate precisely on the restriction. In general terms MET involves placing the joint in question at the limit of its possible motion, in the direction in which it is most restricted. This position is maintained (not exaggerated) by pressure from the practitioner and, in a controlled manner, the patient then attempts to move the joint, by sustained effort, against the practitioner's counterforce. No movement should take place during repeated short or long efforts of this type. After each such effort the joint should be reassessed, and if the range of movement has increased then the joint should be taken to this new limit before the next attempt. This method is virtually painless, and is suitable for self-use in many areas of the body (fingers or elbow, for example).
Muscle Energy Technique (MET) is a further method of applying direct action to a restricted area. With MET, however, it is the patient's own forces which produce the manipulative effort. By placing a joint in a precise position, and calling on the patient to use a muscular effort in a particular direction, against a distinctly executed counter-force from the practitioner, it is frequently possible to achieve dramatic improvements in joint mobility. The skill in such a manouevre is in creating a balance of forces which can operate precisely on the restriction. In general terms MET involves placing the joint in question at the limit of its possible motion, in the direction in which it is most restricted. This position is maintained (not exaggerated) by pressure from the practitioner and, in a controlled manner, the patient then attempts to move the joint, by sustained effort, against the practitioner's counterforce. No movement should take place during repeated short or long efforts of this type. After each such effort the joint should be reassessed, and if the range of movement has increased then the joint should be taken to this new limit before the next attempt. This method is virtually painless, and is suitable for self-use in many areas of the body (fingers or elbow, for example).
Curing Elbow Pain through Osteopathic Manipulative Treatment(OMT)
Source: www.healthlibrary.com/reading/cure/chap13.html
A patient may complain that he cannot pour a cup of tea for himself He experiences difficulty in closing his fist tightly, or while grabbing and lifting heavy things from the ground with his hands. He has pain on the lateral aspect of the elbow at a prominent point called the lateral condyl of the humerus or arm bone. The pain travels along the back of the forearm and may go as far as the wrist or the back of the hand as far as the ring finger of the hand. It may be severe enough to go to the external aspect of the arm up to the shoulder, but this is less common. Sometimes, there is a constant ache, which gets worse at night, disturbing the sleep. The patient may wake up with stiffness of the elbow.
Tennis Elbow
Pain at the elbow joint is commonly seen among tennis players. That is why this condition is commonly called tennis elbow. Those who do not play tennis may also suffer from elbow pain.
The pain starts due to a strain where the wrist has to be extended again and again as is done while playing tennis or while using the hammer. The patient does not feel any pain even after a slight injury to the elbow joint is sustained during these movements. Later on, certain movements at the wrist joint or elbow start hurting and a fortnight later, a tennis player cannot hit backstrokes at all.
It is not the tear of the tendon which causes the pain. The pain is due to the formation of a painful scar which results from multiple injuries. During the game or due to the active use of the elbow and wrist, the healing process which is accelerated by rest and avoidance of movement, remains incomplete. The strain on the extension ligaments is caused during the extension or backward bending at the wrist joint. The pain is peculiar; occasionally it comes on suddenly and the grip of the hand becomes powerless momentarily. The patient may even drop light objects that he is holding on the ground.
Getting a tennis elbow is frequent between the ages of forty to sixty years, the years when cervical spondylosis is also common. A view is often expressed that elbow pain has some relation with the neck. Sometimes this is true. Pain in the elbow joint can arise from the neck without any injury at the elbow. All cases of elbow pain should be examined for a neck lesion too. Generally tenderness can be located at the level of the fifth, sixth and seventh cervical vertebrae. Marked tenderness is noted in the lower part of the neck on the side of the elbow involved. So if the pain in the elbow joint is due to the neck, manipulation of the latter will result in a spectacular recovery. A distinction must be made between elbow pain due to the cervical spine and pain due to a tennis elbow. Sometimes an elbow pain is due to both a cervical lesion and periarthritis of the elbow. These two causes can be easily distinguished. In a true tennis elbow, the extension of the wrist joint is painful. During this test the elbow must be fully stretched. In a true tennis elbow, the side bending of the wrist towards the thumb side is also painful. Sometimes muscles on the lateral aspect of the forearm feel tender on deep palpation; these muscles help in extension at the wrist joint.
Treatment
A tennis elbow recovers on its own without any treatment in about a year, if a person is under sixty years. However it takes longer when the person is over sixty.
Ordinarily it is treated by local hydrocortisone injections. These injections inhibit spontaneous recovery. It is not uncommon for patients to remain well after an injection for a few months and then feel the need for further injections month after month. If left untreated however, there is a possibility that the patient may recover completely in twelve months on It’s own.
Manipulation
Manipulation is found to be effective for a tennis elbow. The elbow is fixed and deep friction is applied on the epicondyl for five to ten minutes before manipulation, This softens the scar tissue which becomes easier to break by manipulation. Manipulation is repeated once or twice a week for four to six weeks. Such sessions are enough to relieve the pain completely. Manipulation is done in hypertension. One may hear the cracking sound during manipulation and relief is felt immediately following the manipulation.
Manipulation shortens the time required for recovery, and once the condition is cured, it does not recur.
Case Histories
A fifty-two-year old man with a good build, employed as a supervisor in building construction, had pain in the elbow for two months. He used to drive a motor cycle for an average of 100 km daily. But the pain made him incapable of driving., He even had a lot of difficulty in lifting and moving the telephone. He had stiffness in the elbow in the mornings, and was not able to sleep well due to the pain. He had had a similar pain earlier on and it had subsided with local injection of hydrocortisone.
X-rays and laboratory tests were conducted after the problem was diagnosed as a tennis elbow. He felt relief after the first manipulative treatment. The pain decreased gradually and subsided six weeks later. He was advised to use his arm as little as possible during the treatment. He never complained of pain for two years following the treatment.
A forty-one-year old housewife with five children had pain in the right elbow for five years. The pain had begun following a fall where she had supported herself by the hand. There was a slight swelling over the elbow. She experienced more pain if she used her hand more during work. Sometimes she felt pain in the forearm and upper arm upto the shoulder and neck.
She came to me with the above-mentioned complaint. There was a slight swelling over her left elbow. The X-ray showed no abnormality and the laboratory tests were normal.
Manipulation of the left elbow was started, along with manipulation of the cervical spine. She felt better following the first treatment. By the third week she was comfortable. The pain became more localized, and there was no pain in the neck and shoulder. The pain in the elbow subsided gradually and in ten weeks she was free of it.
A patient may complain that he cannot pour a cup of tea for himself He experiences difficulty in closing his fist tightly, or while grabbing and lifting heavy things from the ground with his hands. He has pain on the lateral aspect of the elbow at a prominent point called the lateral condyl of the humerus or arm bone. The pain travels along the back of the forearm and may go as far as the wrist or the back of the hand as far as the ring finger of the hand. It may be severe enough to go to the external aspect of the arm up to the shoulder, but this is less common. Sometimes, there is a constant ache, which gets worse at night, disturbing the sleep. The patient may wake up with stiffness of the elbow.
Tennis Elbow
Pain at the elbow joint is commonly seen among tennis players. That is why this condition is commonly called tennis elbow. Those who do not play tennis may also suffer from elbow pain.
The pain starts due to a strain where the wrist has to be extended again and again as is done while playing tennis or while using the hammer. The patient does not feel any pain even after a slight injury to the elbow joint is sustained during these movements. Later on, certain movements at the wrist joint or elbow start hurting and a fortnight later, a tennis player cannot hit backstrokes at all.
It is not the tear of the tendon which causes the pain. The pain is due to the formation of a painful scar which results from multiple injuries. During the game or due to the active use of the elbow and wrist, the healing process which is accelerated by rest and avoidance of movement, remains incomplete. The strain on the extension ligaments is caused during the extension or backward bending at the wrist joint. The pain is peculiar; occasionally it comes on suddenly and the grip of the hand becomes powerless momentarily. The patient may even drop light objects that he is holding on the ground.
Getting a tennis elbow is frequent between the ages of forty to sixty years, the years when cervical spondylosis is also common. A view is often expressed that elbow pain has some relation with the neck. Sometimes this is true. Pain in the elbow joint can arise from the neck without any injury at the elbow. All cases of elbow pain should be examined for a neck lesion too. Generally tenderness can be located at the level of the fifth, sixth and seventh cervical vertebrae. Marked tenderness is noted in the lower part of the neck on the side of the elbow involved. So if the pain in the elbow joint is due to the neck, manipulation of the latter will result in a spectacular recovery. A distinction must be made between elbow pain due to the cervical spine and pain due to a tennis elbow. Sometimes an elbow pain is due to both a cervical lesion and periarthritis of the elbow. These two causes can be easily distinguished. In a true tennis elbow, the extension of the wrist joint is painful. During this test the elbow must be fully stretched. In a true tennis elbow, the side bending of the wrist towards the thumb side is also painful. Sometimes muscles on the lateral aspect of the forearm feel tender on deep palpation; these muscles help in extension at the wrist joint.
Treatment
A tennis elbow recovers on its own without any treatment in about a year, if a person is under sixty years. However it takes longer when the person is over sixty.
Ordinarily it is treated by local hydrocortisone injections. These injections inhibit spontaneous recovery. It is not uncommon for patients to remain well after an injection for a few months and then feel the need for further injections month after month. If left untreated however, there is a possibility that the patient may recover completely in twelve months on It’s own.
Manipulation
Manipulation is found to be effective for a tennis elbow. The elbow is fixed and deep friction is applied on the epicondyl for five to ten minutes before manipulation, This softens the scar tissue which becomes easier to break by manipulation. Manipulation is repeated once or twice a week for four to six weeks. Such sessions are enough to relieve the pain completely. Manipulation is done in hypertension. One may hear the cracking sound during manipulation and relief is felt immediately following the manipulation.
Manipulation shortens the time required for recovery, and once the condition is cured, it does not recur.
Case Histories
A fifty-two-year old man with a good build, employed as a supervisor in building construction, had pain in the elbow for two months. He used to drive a motor cycle for an average of 100 km daily. But the pain made him incapable of driving., He even had a lot of difficulty in lifting and moving the telephone. He had stiffness in the elbow in the mornings, and was not able to sleep well due to the pain. He had had a similar pain earlier on and it had subsided with local injection of hydrocortisone.
X-rays and laboratory tests were conducted after the problem was diagnosed as a tennis elbow. He felt relief after the first manipulative treatment. The pain decreased gradually and subsided six weeks later. He was advised to use his arm as little as possible during the treatment. He never complained of pain for two years following the treatment.
A forty-one-year old housewife with five children had pain in the right elbow for five years. The pain had begun following a fall where she had supported herself by the hand. There was a slight swelling over the elbow. She experienced more pain if she used her hand more during work. Sometimes she felt pain in the forearm and upper arm upto the shoulder and neck.
She came to me with the above-mentioned complaint. There was a slight swelling over her left elbow. The X-ray showed no abnormality and the laboratory tests were normal.
Manipulation of the left elbow was started, along with manipulation of the cervical spine. She felt better following the first treatment. By the third week she was comfortable. The pain became more localized, and there was no pain in the neck and shoulder. The pain in the elbow subsided gradually and in ten weeks she was free of it.
AOA to Promote Preventive Health Issues
Source: AOA Daily Reports

The American Osteopathic Association (AOA) has received a free, 115 square foot window space in Rockefeller Plaza, steps from the NBC Today Show, through Executive Health Exams International (EHE). EHE is a preventive healthcare organization that provides the window space free of charge to a different organization each month to promote preventive health care issues. In January, the AOA will use the space to promote preventive health issues related to obesity, smoking and depression. The display will be available January 3-31st 2006. Rockefeller Center Management estimates the number of people that pass through the Plaza each day as 250,000, providing the AOA with a great opportunity to promote D.O.s/osteopathic medicine.
Subscribe to:
Posts (Atom)